TMS vs. Medication: Which Depression Treatment Is Right for You?
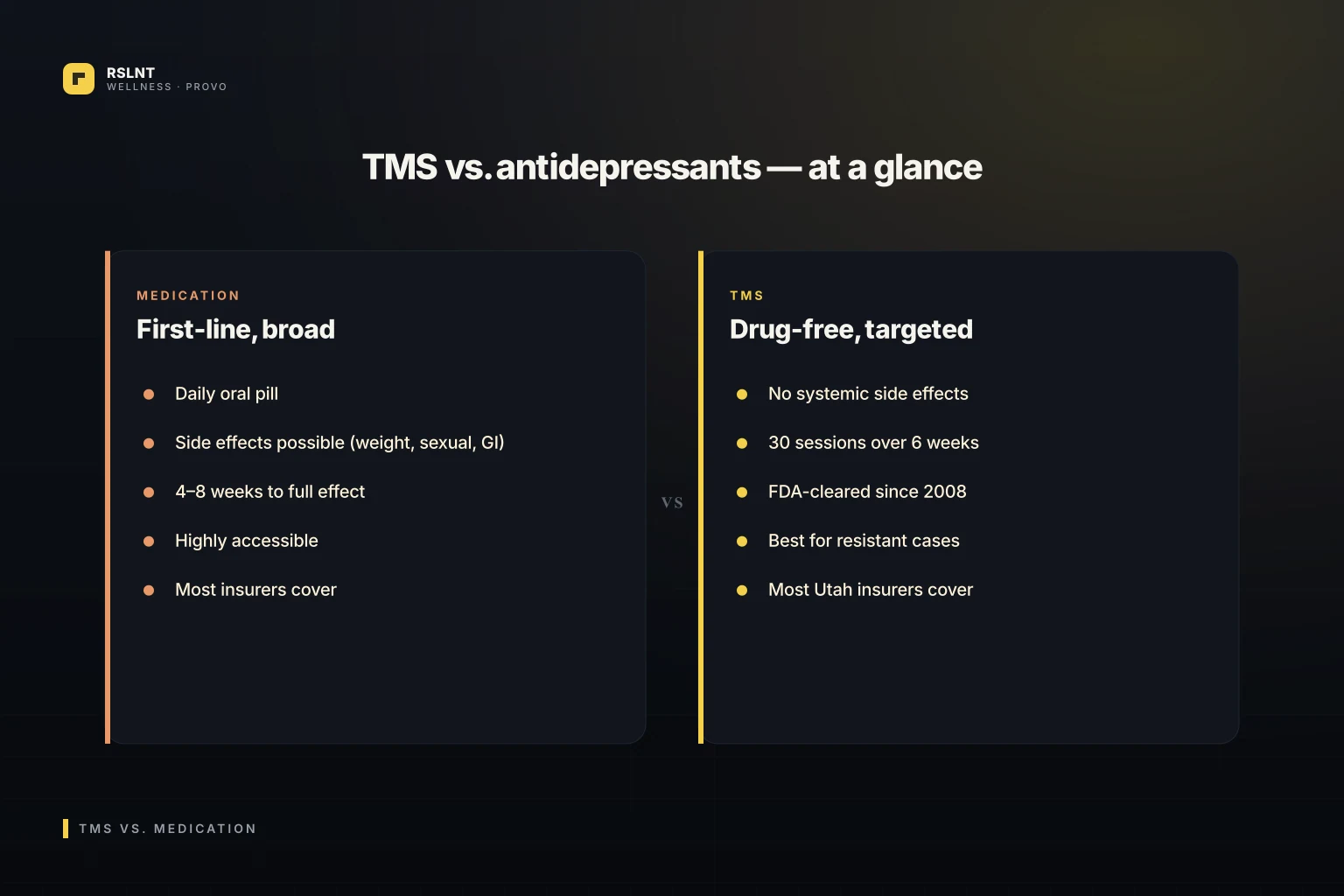
Table of contents
You've been on antidepressants for two years. Maybe three. Maybe seven. Some of them helped a little. Some did nothing. One of them made you gain 25 pounds. Another one numbed everything below the waist.
Now somebody mentioned TMS, and you're sitting at your kitchen table trying to figure out whether you should give the pills another shot or try something completely different.
The short answer. Antidepressants are first-line because they're affordable, widely covered, and work for around 60 percent of patients within 6 to 8 weeks. TMS is the strongest non-medication option for the patients in the other 40 percent. If two or more antidepressants haven't given you full relief, TMS is the next step backed by the FDA, the American Psychiatric Association, and Medicare. It works in 60 to 65 percent of patients who didn't respond to medication. And it has none of the typical antidepressant side effects.
How antidepressants actually work
The most prescribed antidepressants are SSRIs, like sertraline (Zoloft), escitalopram (Lexapro), and fluoxetine (Prozac). They prevent serotonin from being reabsorbed too quickly between neurons, leaving more of it available in the synapse.
The newer family is SNRIs, like venlafaxine (Effexor) and duloxetine (Cymbalta), which work on serotonin and norepinephrine.
The outlier is bupropion (Wellbutrin), which works on dopamine and norepinephrine, and is often used when fatigue and motivation are the dominant symptoms.
These medications work for a real majority of patients. According to the American Psychiatric Association, around 50 to 60 percent of patients respond to the first or second medication tried. The rest don't, and that's where the term treatment-resistant depression comes from.
How TMS actually works
TMS is short for transcranial magnetic stimulation. It's an FDA-cleared medical device that uses pulsed magnetic fields, similar in strength to an MRI, to stimulate the dorsolateral prefrontal cortex, the part of the brain that handles mood, motivation, and emotional regulation.
The device sits on a chair-arm. A coil rests against the side of your head. The coil pulses for about 19 minutes per session. You feel a tapping. You can read or scroll your phone. You can drive yourself home.
The pulses don't cross any blood-brain barrier. There's no medication in your system. The brain responds to repeated stimulation by strengthening its own underactive networks, a process called neuroplasticity.
The FDA cleared TMS for major depressive disorder in 2008 and for OCD in 2018.
The differences that matter
Cost-wise, antidepressants are far cheaper. A generic SSRI runs $4 to $30 a month. TMS without insurance runs $10,000 to $15,000 per course. With insurance, most patients pay $0 to $1,800 out of pocket.
Time-wise, antidepressants take 4 to 6 weeks to start working. A full TMS course runs 6 weeks. So both have a similar runway, but TMS has a clear endpoint. Antidepressants are usually a long-term commitment of 1 to 2 years minimum.
Side effects matter most for people who've already failed antidepressants. Common antidepressant side effects:
- Weight gain
- Sexual dysfunction
- GI distress, especially the first few weeks
- Emotional blunting
- Sleep disruption either way (too sleepy or too wired)
- Possible discontinuation symptoms when tapering
TMS side effects:
- Mild scalp tenderness during the first week
- Tension headache, treatable with Tylenol
- Less than 0.1 percent risk of seizure (mostly in patients with seizure history, who are screened out)
For people who couldn't tolerate medication, that side effect profile is the entire conversation.
Who fits each treatment
Antidepressants make sense if:
- This is your first depressive episode and you haven't tried medication
- You can tolerate the time and side-effect profile
- You're looking for the most affordable option
- You're stable enough to wait 4 to 6 weeks for the first signal
TMS makes sense if:
- You've tried two or more antidepressants without enough relief (this is the FDA indication)
- Past medications had side effects that were untenable
- You're in recovery from substance use and want a drug-free option
- You're already on multiple medications and don't want to add more
- You've completed therapy and need a different lever
- You're a veteran or older patient with a heavy medication stack
These aren't mutually exclusive. Many patients stay on a low-dose SSRI during TMS and continue it after, especially if it gave them partial relief.
What the research actually shows
Multi-site clinical trials and the OPT-TMS trial published in the Archives of General Psychiatry showed response rates of around 30 to 40 percent and remission rates of around 25 percent for TMS in treatment-resistant depression. Real-world clinical numbers are higher, with roughly 60 to 65 percent of patients responding and 30 to 40 percent fully remitting.
For comparison, the STAR*D trial, the largest depression treatment study ever run, showed that after one antidepressant trial, around 30 percent of patients reach remission. After a second, 25 percent of those remaining. The numbers drop with each subsequent medication.
If you've already tried two or three medications, TMS gives you better odds than another medication trial.
How we actually treat this at RSLNT
At RSLNT Wellness, we don't pick treatments by ideology. We pick them by fit.
Counseling alongside whatever you're doing. Cognitive behavioral therapy and acceptance and commitment therapy work well alongside both medication and TMS. We integrate, not silo.
Medication management when you haven't fully explored that path. SSRIs, SNRIs, bupropion, and others depending on history. We don't push pills. We don't withhold them either.
TMS therapy when medication has been tried and hasn't been enough. FDA-cleared, drug-free, six-week course. We handle the prior authorization with your insurer. Most patients pay $0 to $1,800 out of pocket after coverage.
The right answer is sometimes one path. Sometimes it's both at once. We figure that out with you.
Frequently asked questions
Can I stay on my antidepressant during TMS?
Yes. Most patients do. Stopping a medication suddenly carries its own risk, and TMS doesn't interact with antidepressants. We coordinate any tapering later, only if and when it makes clinical sense.
What's the failure rate for both?
Antidepressants have around a 40 to 50 percent rate of insufficient response after one trial. TMS responds in 60 to 65 percent of treatment-resistant patients. If TMS fails, we discuss other options including different medications, ECT for severe cases, or combination therapy.
How do I know which to try first?
If you haven't tried any antidepressant and your symptoms are mild to moderate, start with a medication trial. If you've already tried two or more and they didn't work, TMS is the more evidence-based next move.
Stop guessing. Start with a real assessment.
You've spent enough time alone with this decision.
Schedule a free 15-minute consult. We'll review what you've tried, what's still hard, and which direction makes sense for your specific brain and your specific history. No pressure to commit on the call.
I'm not a therapist or a doctor. I'm someone who went from suicidal ideation, major depressive disorder, and crippling anxiety to clarity of mind. I feel like I got my life back. RSLNT Wellness is the place that helped me get there. If you're struggling, you don't have to figure this out alone.
Frequently Asked Questions
Can I stay on my antidepressant during TMS?
What's the failure rate for both?
How do I know which to try first?
Sources & Further Reading
Every clinical claim in this article is backed by a public, peer-reviewed, or government source. We do not cite anything we cannot link to.
- [1]AntidepressantsMedlinePlusBacks: SSRIs like sertraline, escitalopram, and fluoxetine work by blocking serotonin reuptake.
- [2]AntidepressantsMedlinePlusBacks: SNRIs such as venlafaxine and duloxetine affect both serotonin and norepinephrine.
- [3]BupropionMedlinePlusBacks: Bupropion is an antidepressant used to treat depression.
- [4]Transcranial magnetic stimulation - Mayo ClinicMayo ClinicBacks: TMS is a noninvasive treatment that uses magnetic fields to stimulate nerve cells in the brain.
- [5]Transcranial magnetic stimulation - Mayo ClinicMayo ClinicBacks: TMS is generally used when other depression treatments haven't been effective.
- [6]510(k) Premarket NotificationU.S. Food and Drug Administration · 2008Backs: The NeuroStar TMS Therapy System was FDA-cleared in 2008 for major depressive disorder.
- [7]FDA permits marketing of transcranial magnetic stimulation for treatment of obsessive compulsive disorderU.S. Food and Drug Administration · 2018Backs: The FDA permitted marketing of TMS for obsessive compulsive disorder in 2018.
Ready to feel like yourself again?
Schedule a free consultation to see if TMS therapy is right for you.
Book Your Consultation